Prefinal long case
NOTE: THIS IS AN ONLINE E LOGBOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS/HER GUARDIAN'S SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH A SERIES OF INPUTS FROM THE AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS INTENDING TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE-BASED INPUT.
This is a case of 25yr old male came from narketpally,car driver by occupation
Cheif complaints: generalised weakness since 3months
Hopi:
3months ago he developed increased frequency of urination (also nocturia) also he has generalised weakness after 10days of developing weakness he went to the local hospital where he was diagnosed with diabetes , doctor prescribed medication then he took rest for 10days (where his weakness got subsided even though he has increased frequency of urination
15days back his frequency of urination was subsided
After completion of 10days he went to his work (he drives 4-5hrs in a day) he again developed generalised weakness even though he didn't stop driving due to financial crisis
He had 2-3 episodes of head ache throbbing type of pain relived by medication associated with neck pain
He changed his diet plan after diagnosis . he takes roti (2 times in a day), afternoon he eats fruits .his appetite decreased due to nausea
Tingling sensation since 3months over the sole
H/o Weight loss 2-3kgsince3months
Yellowish discoloration of urine since 2 days
Blurring of vision since 2days
Past history:not a known case of htn, epilepsy,TB, thyroid abnormalities,no surgeries
Personal history:diet -mixed
Appetite -normal
Bowel and bladder movements are regular
Sleep -adequate
Occasionally he drinks alochol (in family function)
Family history:his 50yrs old father has diabetes since 5yrs
General examination:-
Patient is conscious, coherent, cooperative well oriented to time place and person .
Moderately built, moderately nourished
His mid arm circumference -12cm
Abdominal circumference -35cm




Pallor:- absent

Icterus:- absent

Cyanosis:- absent
Clubbing:- absent
Generalized lymphadenopathy:- absent
Bilateral pedal edema :- absent
Per abdomen:
On Inspection
Shape of abdomen :-flat
Umbilicus is inverted.
No scars , engorged veins.
All parts of abdomen are moving equally with respiration
On palpation:- all inspectory findings are confirmed.
abdomen is soft, non tender
On bimanual examination of kidney- kidney are not palpable.
On percussion:- no shifting dullness and no fluid thrills.
On auscultation:- normal bowel sounds are heard
Respiratory examination:
Shape of chest-elliptical
Trachea-central
Bilateral air entry present
Vesicular breath sounds are heard
No added sounds
Cvs:
Apical impulse present
S1,s2 are heard
CNS: higher mental functions intact
Rt. Lt
Bulk: Normal Normal
Tone:
Upperlimb. Normal. Normal
Lowerlimb. Normal Normal
Reflexes: biceps. +. +
Triceps. +. +
Supinator. +. +
Knee. +. +
Ankle. + +
Sensory examination
Spinothalamic tract
Crude touch
Rt. Lt
Upper limb -Normal Normal
Lower limb- normal normal
Pain
Upper limb Normal Normal
Lower limb normal
Temperature
Upper limb Normal Normal
Lower limb normal normal
Posterior column
Fine touch. Rt. Lt
Upper limb Normal Normal
Lower limb normal normal
Vibrations. Normal
Cortical
Tactile localisation
Rt. Lt
Upper limb Normal Normal
Lower limb normal normal
Joint sense:normal
Two point discrimination:normal
Stereognosis
Upper limb Normal Normal
meningeal signs absent
Provisional diagnosis:type 1 diabetes mellitus with hypertryglyceridemia






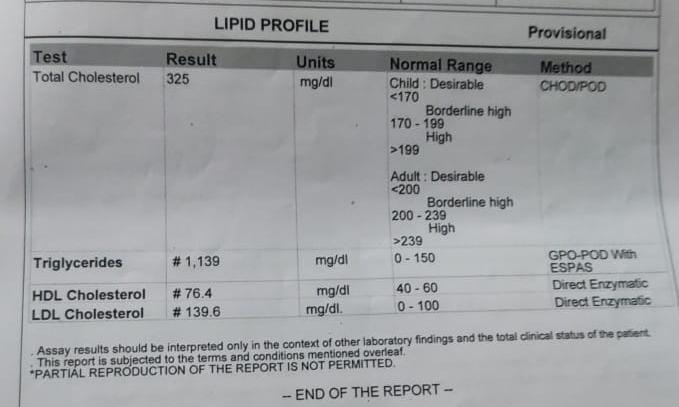





Plbs-208mg/dl

Comments
Post a Comment